Neuro Oncol. 2012 Oct 25. [Epub ahead of print]
A phase I/II trial of vandetanib for patients with recurrent malignant glioma.
Kreisl TN, McNeill KA, Sul J, Iwamoto FM, Shih J, Fine HA.
Source
Neuro-Oncology Branch, National Cancer Institute, National Institutes of Health, Bethesda, Maryland (T.K., K.M., F.I., J.S., H.F.); Biometric Research Branch, Division of Cancer Treatment and Diagnosis, National Cancer Institute, Bethesda, Maryland (J.S.).
Abstract
Vandetanib is a once-daily multitargeted tyrosine kinase inhibitor of vascular endothelial growth factor receptor-2, epidermal growth factor receptor, and the rearranged-during-transfection oncogene. A phase I trial was conducted to describe the pharmacokinetics of vandetanib in patients with recurrent glioma on enzyme-inducing anti-epileptic drugs (EIAEDs) and to identify the maximum tolerated dose (MTD) in this population. A phase II trial evaluated the efficacy of vandetanib in patients with recurrent malignant glioma not on EIAEDs as measured by 6-month progression-free survival (PFS6). In the phase I trial, 15 patients were treated with vandetanib at doses of 300, 400, and 500 mg/day, in a standard dose-escalation design. The MTD in patients on EIAEDs was 400 mg/day, and steady-state levels were similar to those measured in patients not on EIAEDs. Dose-limiting toxicities were prolonged QTc and thromboembolism. Thirty-two patients with recurrent glioblastoma multiforme (GBM) and 32 patients with recurrent anaplastic gliomas (AGs) were treated in the phase II trial, at a dosage of 300 mg/day on 28-day cycles. Six patients (4 GBM, 2 AG) had radiographic response. PFS6 was 6.5% in the GBM arm and 7.0% in the AG arm. Median overall survival was 6.3 months in the GBM arm and 7.6 months in the AG arm. Seizures were an unexpected toxicity of therapy. Vandetanib did not have significant activity in unselected patients with recurrent malignant glioma.
|
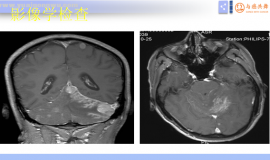
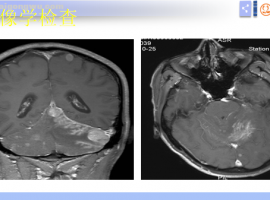 脑膜转移诊疗潘振宇教授科普总结
脑膜转移诊疗潘振宇教授科普总结
脑膜转移 中位治疗生存期 3-6月
脑膜转移的临床表现
脑膜转移诊疗潘振宇教授科普总结
脑膜转移诊疗潘振宇教授科普总结
脑膜转移 中位治疗生存期 3-6月
脑膜转移的临床表现
 肺腺癌egfr19+骨转移,这样治疗可以
病情与治疗过程概述
患者年龄58岁,男性,已戒烟30年
1. 确诊情况(2025.05.26):患
肺腺癌egfr19+骨转移,这样治疗可以
病情与治疗过程概述
患者年龄58岁,男性,已戒烟30年
1. 确诊情况(2025.05.26):患
 肿瘤患者出现水肿,11种缓解方法请收
作者:闵水肿是中晚期肺癌患者比较常见的一种副作用,它不仅影响美观,还给不少病友的
肿瘤患者出现水肿,11种缓解方法请收
作者:闵水肿是中晚期肺癌患者比较常见的一种副作用,它不仅影响美观,还给不少病友的
 卡度联合安罗,谁让肿瘤缩小了
肺低分化腺,伴肉瘤样。卡度尼利单抗联合安罗替尼。两个疗程复查显示肿瘤缩小,胸膜增
卡度联合安罗,谁让肿瘤缩小了
肺低分化腺,伴肉瘤样。卡度尼利单抗联合安罗替尼。两个疗程复查显示肿瘤缩小,胸膜增
 父亲确诊“癌王”生命危在旦夕,医护
讲述者:吉吉整理者:pear
一年前,父亲被确诊为胰腺癌伴肝转移,那一刻,我的人生仿
父亲确诊“癌王”生命危在旦夕,医护
讲述者:吉吉整理者:pear
一年前,父亲被确诊为胰腺癌伴肝转移,那一刻,我的人生仿






 显身卡
显身卡