http://www.slideshare.net/JackWe ... ew-ideas-new-agents
1. Acquired Resistance to Targeted Therapies in Advanced Non-Small Cell Lung Cancer: New Strategies and New Agents H. Jack West, MD Medical Director, Thoracic Oncology Program Swedish Cancer Institute Seattle, WA February , 2014
2. Is Acquired Resistance a New Problem? “We’ve always seen acquired resistance before targeted therapies – this isn’t any different from chemo” But… This is a prospectively defined population Response rate 60-75%, often profound Median duration of response 9-13 months This is a distinct clinical entity with its own natural history, reflective of a new era of molecular oncology
3. Case: EGFR Mutation, Isolated Progression • 43 year old never-smoking Caucasian woman with no PMH noted R chest/shoulder pain, also heartburn symptoms that worsened over several weeks. • RUQ U/S shows no abd pathology but R pleural effusion noted • CXR shows effusion and pleural nodules • CT chest – mod to large pleural effusion compressing R middle and lower lobes, 2.5 x 0.7 cm nodule along pleural surface in R midlung, smaller pleural-based nodules elsewhere
4. Case: EGFR Mutation, Isolated Progression • Thoracentesis yields 1700 cc serosang fluid, cytology shows TTF-1 positive adenocarcinoma effusion noted • Cell block: pos for exon 19 mutation in EGFR gene, negative for ALK rearrangement • No other areas of disease noted on PET/CT, brain MRI • She starts erlotinib  marked clinical and radiographic response
5. Case: EGFR Mutation, Isolated Progression • 7 months later, she develops headache and vision changes: head MRI shows 2 cm L occipital lesion & no other lesions • She undergoes gamma knife radiosurgery. What do you recommend for her systemic therapy? A. B. C. D. E. F. No change: continue erlotinib Switch to chemotherapy-based treatment Add chemo to ongoing erlotinib Afatinib Afatinib/cetuximab Send for clinical trial with novel agent
6. Case: EGFR Mutation, Isolated Progression • Would your answer be the same if she had a solitary new lung lesion instead of a solitary brain lesion? A. B. Yes No
7. Acquired Resistance to Targeted Therapy: Heterogeneous Patterns Diverse molecular mechanisms of resistance  diverse clinical patterns of progression • Single focus of progression (still decreased tumor burden vs. pre-targeted therapy) • Slow, minimal multifocal progression (still decreased tumor burden vs. pre-targeted therapy) • Rapid, more diffuse progression (exceeding tumor burden pre-targeted therapy)
8. At Least 3 Clinical Subtypes of Acquired Resistance to Targeted TKIs PD-Subtype CNS-PD (Sanctuary) Oligo-PD Systemic-PD Courtesy of D. Gandara
9. If significant progression, is it isolated or more diffuse? Is “oligoprogression” analogous to oligometastatic/precocious metastatic disease? Perhaps especially for CNS disease – why? • Poor CNS penetration of both EGFR TKIs and crizotinib, so brain mets may not represent resistance to drug (Bronischer CCR, 2007; Costa JCO 2011) • T790M seen in 60% of progressing lesions in acquired resistance, but only 10% of lesions from CNS progression (Hata, ASCO 2012, A#7528)
10. Prolonged Benefit from Rx to Intracranial Mets with Ongoing Targeted Therapy • Growing number of patients who have been continued on EGFR TKI or crizotinib after radiation to brain metastases in absence of extracranial progression - median duration of ongoing response is months - some patients continue to do well without change in systemic therapy for years
11. Local Therapy in Acquired Resistance: University of Colorado Experience • 65 pts (38 ALK+, 27 EGFR mut’n+) of whom 51 (28 ALK, 23 EGFR) progressed • 25 (49%) with CNS (no LMC) or <4 extracranial sites of progression Weickhardt, J Thorac Oncol 2013
12. Local Therapy in Acquired Resistance: Extracranial Oligoprogression • 18/184 pts  local therapy for extracranial PD (CNS PD excluded) • Median time to new systemic Rx: 22 months Yu, J Thorac Oncol 2013
13. Local Therapy for Acquired Resistance • As a proof of principle, a subset of pts can have prolonged non-progression and excellent survival after local therapy • There may still be value in ongoing targeted therapy • Could pts have potentially done just as well by not doing imaging or ignoring the lesion? Is this just favorable natural history? • Only 4 mo median PFS in U. CO experience – perhaps multifocal PD is too liberal • MGH applied this approach to only 10% of AR pts • Criteria need to be defined before broad adoption
14. Case: EGFR Mutation, Multifocal Progression • 70 year old Indian maintenance man with remote prior smoking history (8 pack-years, quit 45 years ago) • Presented with cervical LAN that ultimately proved to be benign, but he’s found to have 2.5 cm RUL moddifferentiated adenocarcinoma  resected • 8 months after surgery, he’s found to have multifocal recurrence in lungs bilaterally • Biopsy confirms lung adenocarcinoma, EGFR activating mutation in exon 19 • Starts erlotinib and responds with good PR
15. Case: EGFR Mutation, Mild progression • 11 months later, several of the lung lesions appear to have grown by about 1-2 mm, though still smaller than pre-treatment baseline. He feels well. • What do you recommend for his systemic therapy? A. No change: continue erlotinib B. Switch to chemotherapy-based treatment C. Add chemo to ongoing erlotinib D. Afatinib E. Afatinib/cetuximab F. Send for clinical trial
16. Case: EGFR Mutation, Subsequent Course & Faster Progression • He continues on erlotinib, and follow up scan 2 months later demonstrates minimal progression. He remains asymptomatic. • Unfortunately, after another 2 month interval, his scan shows that he has multiple new lung lesions and most existing ones have grown significantly. • What do you recommend for his systemic therapy? A. Switch to chemotherapy-based treatment B. Add chemo to ongoing erlotinib C. Afatinib D. Afatinib/cetuximab
17. Does Detectable Progression Require a Treatment Change? Disease burden Time NOT necessarily clinically significant progression
18. What DOESN’T Constitute Clinically Significant Progression? Mild increase in metabolic activity on PET Rising serum tumor marker Slow, slight increase in tumor size (1-2 small new nodules against background of excellent disease control?)
19. Concurrent TKI and chemo-based Therapy Treating distinct cancer cell populations Risk of “flare response”/rebound progression Disease burden D/C targeted Rx continue targeted Rx Time TKI sensitive TKI sensitive TKI resistance TKI sensitive TKI resistance
20. Rapid Progression with Discontinuation of EGFR TKI after Prolonged PFS Rapid acceleration of PD  hospitalization and/or death after discontinuation of EGFR seen in up to ~1/4 of pts in MSKCC series (Chaft, Clin Cancer Res, 2011) Last day of TKI Off EGFR TKI Resumed TKI Day 0 Day 21 Day 42 Also reported after discontinuation of crizotinib after acquired resistance in ALK-positive NSCLC (Pop, J Thorac Oncol, 2012)
21. For Cancers with a Known Driver Mutation, Continuing Inhibition of that Target is Beneficial after Progression • Progression of CML on imatinib  increase dose, or dasatinib, or nilotinib lead to consistent response • Solid tumor example: HER2+ breast cancer Von Minckwitz, JCO 2009
22. Treatment Options after Acquired Resistance to EGFR (or other) TKI Oxnard, Clin Cancer Res, 2011
23. Continued treatment beyond progression, Dana Farber Experience • 42 EGFR mutn-pos pts s/p 1st line erlotinib on one of 3 clinical trials • 45% continued without significant progression > 3 months • 21% required no further treatment change for > 12 months Oxnard, ASCO 2012, A#7524
24. Chemo/Erlotinib vs. Chemo Alone at Progression after Acquired Resistance • N = 78 retrospective review of outcomes – chemo alone (N = 44) or – chemo/erlotinib (N = 34) • RR 18% (chemo) vs. 41% with chemo/erlotinib) • No differences in PFS or OS between these two strategies Goldberg, ASCO 2012, A#7524
25. Prospective Rand Ph 2 Rand Trial Suggests No Benefit to Treatment Beyond Progression • N = 39 pts w/clin benefit after >12 weeks erlotinib, then PD • EGFR mutation not required; CR/PR not required • Randomized to chemo (pem or docetaxel) +/- erlotinib • Closed due to slow accrual Progression-Free Survival Chemo alone Chemo/erlotinib Halmos, ASCO 2013, A#8114 Overall Survival Chemo alone Chemo/erlotinib
26. Chemo with Concurrent EGFR TKI • Studies in unselected or clinically selected populations show no benefit but no signal of increased harm • Combinations of chemo and TKIs are certainly feasible • Little prospective study in setting of acquired resistance yet • ph II trial of pem/EGFR TKI as 3rd line (Yoshimura, JTO 2013) • N = 27; RR 26%, DCR 78%, med PFS 7.0 mo, med OS 11.4 mo • Unclear if they are significantly more favorable than chemo alone in acquired resistance
27. Chemotherapy +/- Ongoing EGFR TKI for Acquired Resistance IMPRESS TRIAL PI: Tony Mok & Jean-Charles Soria Activating EGFR mutation Progression on gefitinib No prior chemotherapy N = 250 R A N D Primary endpoint: progression-free survival Cisplatin/Pemetrexed Cisplatin/Pemetrexed + ongoing gefitinib
28. Chemotherapy +/- Ongoing EGFR TKI for Acquired Resistance, with Retreatment PI: Leora Horn (Vanderbilt) Advanced NSCLC Activating EGFR mutation Resp to EGFR TKI>4 mo No prior chemotherapy PS 0/1 N = 120 R A N D Cis or Carbo/Pemetrexed + ongoing erlotinib Cis or Carbo/Pemetrexed Stratification by: EGFR mut’n exon 19 vs. exon 21 Time to progression on EGFR TKI <1 yr vs. >1 yr PS 0 vs. 1 Primary endpoint: progression-free survival Erlotinib re-treatment
29. Chemo Without TKI Can Be Followed by Re-treatment Oxnard, Clin Cancer Res, 2011
30. Activity of EGFR TKIs on Re-Challenge • Many small series published: RR<10%, PFS <4 months • Minority of patients can demonstrate significant tumor shrinkage • Larger subset will have stability again for many months • Reacquisition of TKI sensitivity, loss of T790M, etc., most notably in patients off targeted therapy for 6-12 months or longer • Seen after crizotinib re-challenge as well (Browning, JTO 2013) • Is this meaningfully beneficial? If so, is this as good as, better than, or worse than ongoing treatment beyond progression?
31. EGFR TKI Re-treatment after Acquired Resistance: DFCI/MGH Experience • Retrospective, 24 pts (over 9.5 yrs) with activating EGFR mutation after AR to gefitinib (30%) or erlotinib (70%) • RR 4%, SD 63% • Median interval off EGFR TKI 5 mo (range 2-46 mo) • Greater benefit w/longer interval of EGFR TKI (PFS 4.4 vs. 1.9 mo for 6 mo interval off EGFR TKI) Heon, ASCO 2012, A#7525
32. Re-challenge with EGFR TKI after Acquired Resistance • N = 73 pts with acquired resistance • OS post-PD better for 56 who had EGFR TKI re-administered vs. 17 who did not • No correlation of benefit w/interval off EGFR TKI seen Hata, ASCO 2012, A#7528
33. Mechanisms of Acquired Resistance in EGFR Mutation-Positive Disease: Repeat Biopsies? • SCLC in 3-15% • Otherwise, rare to find actionable result with current approved agents Paired biopsies (N=106) • May provide some insight about prognosis (+/- value of ongoing TKI?) Oxnard, Clin Cancer Res, 2011 Repeat biopsies are not standard of care and have a relatively low probability of being immediately actionable, but they are likely to drive our understanding and future treatments in this setting.
34. Novel Agents: Irreversible TKIs in Clinical Trials • HKI-272 (EGFR + Her2) • RR 2% in TKI-resistant patients • Intriguing responses in G719X patients (Sequist, JCO 2010) • Cabozantinib (EGFR, Her2, VEGF) • RR 2% in TKI-resistant patients (Pennell, Chicago Lung ’08) • Dacomitinib (EGFR + Her2) • RR 7% in TKI-resistant patients (Janne, ASCO ’09) • Afatinib (EGFR + Her2) • RR 7% in TKI-resistant pts, 2 mo PFS improvement (Miller, Lancet Oncol 2012)
35. LUX Lung 1 Patients with: • Adenocarcinoma of the lung • Stage IIIB/IV • Progressed after one or two lines of chemotherapy (incl. one platinum-based regimen) and ≥12 weeks of treatment with erlotinib or gefitinib • ECOG 0–2 N=585 Randomization 2:1 Oral BIBW 2992 50 mg once daily plus best supportive care Oral placebo once daily plus best supportive care Primary endpoint: Overall survival (OS) Secondary: PFS, RECIST response, QoL, safety Miller, Lancet Oncol 2012
36. LUX Lung 1: Efficacy Progression-Free Survival Miller, Lancet Oncol 2012 Overall Survival
37. Afatinib + Cetuximab in EGFR-mutated NSCLC refractory to EGFR TKI N = 60 Response rate: 30% Clinical benefit (DCR): 75% Janjigian, et al. ESMO 2012 • This is specific for afatinib combination: Erlotinib/cetuximab had RR 0/13 (Janjigian, CCR 2011)
38. Trial Concepts: Afatinib + Cetuximab Advanced NSCLC Activating EGFR mutation No prior chemotherapy PS 0-2 SWOG: EGFR TKI-naïve ECOG: Acquired Resistance R A N D Afatinib 40 mg PO daily Afatinib 40 mg PO daily + Cetuximab IV weekly Primary Endpoint: PFS Rebiopsy at progression
39. MISSION Trial of Sorafenib vs. Placebo: PFS based on EGFR mutation status Patients with EGFR mut (in tumor or plasma) Patients with EGFR wild type • Sorafenib N=44; Placebo N=45 • HR=0.27 (95% CI 0.16,0.46) • P-value<0.001 • Sorafenib median PFS= 2.7 mo (83d) • Placebo median PFS= 1.4 mo (42d) • Sorafenib N=122; Placebo N=136 • HR=0.62 (95% CI 0.48,0.82) • P-value<0.001 • Sorafenib median PFS= 2.7 mo (82d) • Placebo median PFS= 1.5 mo (46d) Biomarker treatment interaction analysis: p-value=0.015 Mok, ESMO 2012
40. MISSION Trial of Sorafenib vs. Placebo: OS based on EGFR mutation status Patients with EGFR mut (in tumor or plasma) Patients with EGFR wild type • Sorafenib N=44; Placebo N=45 • HR=0.48 (95% CI 0.3,0.76) • P-value=0.002 • Sorafenib median OS= 13.9 mo (423d) • Placebo median OS= 6.5 mo (197d) • Sorafenib N=122; Placebo N=136 • HR=0.92 (95% CI 0.7,1.21) • P-value=0.559 • Sorafenib median OS= 8.3 mo (253d) • Placebo median OS= 8.4 mo (256d) Biomarker*treatment interaction analysis: p-value=0.023 Mok, ESMO 2012
41. T790M Mutation • May have a better Px than non-T790M mechanisms: 19 vs. 12 mo post-progression N = 93 • T790M more likely to show progression in lungs/pleura • Non-T790M more likely to progress distantly, & with worse PS Oxnard, Clin Cancer Res 2010
42. CO-1686: Oral Inhibitor of EGFR Mutations & T790M Mutations (not EGFR wild type) • 67% response rate in T790M+ patients (WCLC, 2013) – Dosing 900 mg PO BID • No rash (c/w absence of systemic wt EGFR inhibition) Soria, WCLC 2013, Sydney
43. Series of Global Registration Trials for CO-1686 TIGER: Third –gen Inhibitor of Mutant EGFR in Lung CancER • TIGER1: Ph 2/3 rand trial vs. erlotinib in newly Dx’d pts • TIGER2: Ph 2 in 2nd line T790M+ pts w/PD after 1 EGFR TKI • TIGER3: Ph 2 of later T790M+ pts after >1 EGFR TKI or chemo post-progression • TIGER4: Ph 2 in 2nd line or later for T790M+ detected by blood/plasma assay • TIGER5: Ph 3 rand trial vs. chemo in 2nd line or later
44. AZD9291: Preclinical data • AZD9291 is a potent oral, irreversible inhibitor of EGFR that contains EGFRTKI-sensitizing (EGFRm+) and resistance mutations (T790M) • AZD9291 achieved complete and durable response in H1975 xenograft Good potency and high selectivity demonstrated in enzymatic and cellular in vitro assays Model AZD9291 phosphoEGFR IC50 μM Wild-type LoVo cells EGFRm+ PC9 cells EGFRm+/T 790M H1975 cells 0.480 0.017 0.0115 AstraZeneca data on file V, vehicle
45. AZD9291: Best % change from baseline in target lesions 89 patients with documented radiological PD while on EGFR-TKI No DLTs at 20-160 mg/d (dosing to 240 mg/d) No dose reductions Ranson, WCLC 2013, Sydney
46. AZD9291: Clinical response • Patient with Ex19Del & T790M+ pre-gefitinib; PD on gefitinib immediately before AZD9291 • Dose escalation Cohort 1 (20 mg/day) • 24 weeks exposure • No AEs greater than Grade 1 • Ongoing confirmed partial response Preliminary data
47. AUY922: HSP90, “Onco-Chaperone” Inhibitor Johnson, Proc ASCO 2013
48. AUY922/Erlotinib in EGFR Mutation-Positive with Acquired Resistance Johnson, Proc ASCO 2013
49. Acquired Resistance in ALK+ NSCLC: Mechanisms are Diverse ALK resistance mutations ALK amplification Alternative signaling pathways ALK+ • At this time, there is no established role for rebiopsy, but potential to identify bypass tracks
50. Chemotherapy +/- Ongoing Crizotinib for Acquired Resistance in ALK-Positive NSCLC SWOG 1300 PI: Ross Camidge, U Colorado ALK rearrangement Progression on crizotinib After CR/PR or SD>3 mo No prior pemetrexed N = 108 R A N D Pemetrexed + ongoing crizotinib Pemetrexed Primary endpoint: progression-free survival Crizotinib rechallenge
51. Second Generation ALK Inhibitors and IC50s vs. Resistance Mutations --- Approximate steady-state trough concentration at recommended phase 2 dose 10010000 0 N a tivN a tiv e e G A G 1 2 6 91 2 6 9 A IC 5 0 (n M ) IC 5 0 (n M ) 1001000 0 L 1 1 5L 1 1 5 2 R 2R L 1 1 9L 1 1 9 6 M 6M 100100 F 1 1 7F 1 1 7 4 L 4L S Y S 1 2 0 61 2 0 6 Y C Y C 1 1 5 61 1 5 6 Y 10 10 D N D 1 2 0 31 2 0 3 N T 1 1 5T 1 1 5s T in s 1 T in 1 GR G 1 2 0 21 2 0 2 R 1 1 C in ib A 113 C r iz ortiz o t in ib A P 2 6P 2 6 1 1 3 ARIAD Pharmaceuticals LDK C 24802 AS 26 L D K 3 7 83 7 8 C H 5 4H 5 4 2 4 8 0 2 A S P 3 0P 3 0 2 6
52. Activity of Ceritinib in CrizotinibResistant ALK Mutants • Crizotinib resistance mechanisms can be grouped into two broad categories1–3 IC50 Values from Ba/F3 Cellular Assays1 IC50 (nM) Mutation Ceritinib Crizotinib – Alterations in or amplification of the ALK gene Ba/F3 EML4-ALK 20 120 L1152P 180 280 – Bypass mechanisms affecting non-ALK signaling pathways (eg, EGFR, HER2) C1156Y 130 350 I1171T 40 310 F1174C 340 440 L1196M 60 810 G1202R 490 1020 S1206A 150 250 G1269S 140 1600 • Ceritinib is active against many known ALK crizotinib resistance mutations1–3 • In EML4-ALK+ lung cancer xenografts, ceritinib inhibited growth of crizotinib-resistant tumors4 1. 2. 3. 4. Shaw AT et al. J Clin Oncol. 2013;31(suppl):Abstr 8010; Doebele RC et al. Clin Cancer Res. 2012;18:1472-1482; Takeda M et al. J Thoracic Oncol. 2013;8:654-657; Li N et al. Presented at AACR-NCI-EORTC; November 12–16, 2011; San Francisco, CA. Abstr B232.
53. Ceritinib: Activity in Patients with Advanced ALK+ NSCLC
54. Ceritinib: Response in the CNS T1- post T1- post Flair Flair Continued response in CNS at 6 months Baseline After 6 weeks of ceritinib
55. Ceritinib: Ongoing Clinical Trials Trial Description/Setting ClinicalTrials.gov Number Phase Status Ceritinib in previously treated (criz NCT01685060 + chemo) ALK+ NSCLC II Ongoing, not recruiting Ceritinib in crizotinib-naïve ALK+ NCT01685138 II Ongoing Ceritinib vs. chemo in crizresistant ALK+ NSCLC NCT01828112 III Ongoing Expanded access ceritinib in ALK+ NSCLC NCT01947608 NA Ongoing
56. Alectinib (300 mg PO BID) in crizotinib-naïve ALK+ Japanese NSCLC Pts ORR 93.5% (assessment by IRC) Median duration of treatment not yet reached but >14 months Nakagawa, ASCO 2013, A#8033
57. Alectinib in Crizotinib-Refractory ALK+ Non-Japanese Population (N = 47) Gadgeel, WCLC Sydney, 2013, A# O16.06
58. AP26113: ALK+ NSCLC Anti-Tumor Activity Target Lesions (N=34) Best Change from Baseline in Target Lesion (%) Best Overall Response: 58 • 40 20 b Progressive Disease Stable Disease Partial Response Complete Response 65% (22/34) objective response rate (95% CI: 47-80%) • 61% (19/31) post-crizotinib (incl. 1 criz intolerant) • 100% (3/3) in TKI-naïve (incl. 1 CR) 0 -20 -40 a c b -60 a -80 -100 • Response duration 8+ to 40+ weeks • 14 confirmed, 4 awaiting confirmation d a All patients received prior crizotinib unless otherwise indicated; Doses ranged from 60-240 mg/d (23 pts ≥180mg/d); aTKI-naïve; bReceived prior crizotinib and LDK378; cPD by RECIST 1.1 due to 2nd primary tumor of melanoma; dCrizotinib-intolerant Data as of 6 Sept 2013
59. AP26113: ALK+ NSCLC Time on Treatment Discontinued Patients (N=40) On Study • 30/40 (75%) patients still on therapy • 15 ALK+ NSCLC patients have received treatment for at least 6 months, 12 (80%) continue on study 0 10 20 30 40 50 60 70 80 Time on Treatment (Weeks) First dose to last dose if discontinued, first dose to date of data cut if on study Data as of 6 Sept 2013
60. AP26113: Response at 60 mg BID in Crizotinib-resistant ALK+ NSCLC Baseline After 12 Weeks of AP26113 PR is ongoing, 16+ weeks; Images courtesy of Dr. S. Gettinger Data as of 6 Sept 2013
61. AP26113: Brain Metastases Activity Baseline After 8 wks of 180 mg AP26113 Patient 1 Both patients have crizotinibresistant ALK+ NSCLC Patient 2 Images courtesy of Dr. D.R. Camidge Data as of 6 Sept 2013
62. AP26113: Brain Metastases Activity Discontinued Patients On Study 0 10 20 30 40 50 60 Time on Treatment (Weeks) • 8 of 10 ALK+ NSCLC patients with active brain lesions at baseline had evidence of radiographic improvement in brain • Duration of CNS benefita ranging from 8+ to 40+ weeks Data as of 6 Sept 2013
63. HSP90 Chaperone Stabilizes Client Proteins: Inhibitors leads to Client Protein Degradation Proper folding HSP90 binds to client protein >200 client proteins identified. Examples: ALK, AKT, BCR-ABL, BRAF, CDK4, CHK1, EGFR, FLT3, HER2, HIF1α, KIT, MET, PDGFRα, CRAF, SRC, VEGFR, AR, ER … HSP90 inhibitor prevents HSP90 binding to client (competitively binds the ATP pocket of hsp90) Activated client; cell survival, proliferation Inactive client, degraded through proteasome
64. IPI-504 (Retaspimycin): HSP90 Inhibitor Efficacy by ALK FISH Status Sequist, ASCO 2011
65. HSP90 Inhibitor Ganetespib Especially Active in ALK-Positive Patients Wong, ASCO 2011
66. Ganetespib activity in ALK+ NSCLC 24 year old male Chemotherapy, progressed; crizotinib 1 year (PR), progressed Baseline After three weeks (3 doses) ganetespib 66
67. Acquired Resistance: General Principles • No clear evidence-based approaches yet • Conclusions/dogma derived from decades of experience with chemo don’t necessarily apply • Consider local therapy to limited area(s) of PD, especially within the CNS, which may be an issue of drug exposure, not true resistance • Slow progression may not necessitate any change in systemic therapy • Consider rebiopsy: tissue findings have small chance of revealing actionable off-protocol results, are integral for trials in this setting, & will increase our understanding
68. Multiple Options for Acquired Resistance in EGFR Mutation-Positive Advanced NSCLC • Commercially available options – Switch to standard chemotherapy +/- bevacizumab – Add chemo to ongoing EGFR TKI – Afatinib +/- cetuximab (financial toxicity) • Clinical trial options – – – – – Large trials of chemo +/- EGFR TKI beyond progression Afatinib/cetuximab AZ9291 CO1686 AUY922
69. Multiple Options for Acquired Resistance in ALK Rearrangement-Positive Advanced NSCLC • Commercially available options – Switch to std chemo (esp pemetrexed?) +/- bevacizumab – Add chemo to ongoing crizotinib • Clinical trial options – SWOG trial of pemetrexed +/- ongoing crizotinib – – – – Ceritinib (LDK378) Alectinib (CH5424802) AP26113 HSP90 inhibitors |
 求助各位老师,出现甲减,免疫治疗需
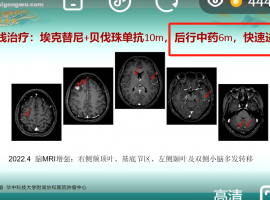
母亲74岁,2025.1.8日确诊中央型肺腺癌IV期,骨转,淋巴结转,纵隔转移,基因检测kras
求助各位老师,出现甲减,免疫治疗需
母亲74岁,2025.1.8日确诊中央型肺腺癌IV期,骨转,淋巴结转,纵隔转移,基因检测kras
 电场治疗癌症业余实现(睡眠专用型)
2025.4.25 增加高电压输出的方案
便携式的肿瘤电场治疗装置已在去年本人所发的帖子中
电场治疗癌症业余实现(睡眠专用型)
2025.4.25 增加高电压输出的方案
便携式的肿瘤电场治疗装置已在去年本人所发的帖子中
 基因检测也会骗人?来个RNA测序试试
作者:潜水
最近,一位肺癌病友告诉笔者,自己做了两次穿刺组织基因检测,都没有任何
基因检测也会骗人?来个RNA测序试试
作者:潜水
最近,一位肺癌病友告诉笔者,自己做了两次穿刺组织基因检测,都没有任何
 感慨!!!一个非常令人伤感的病例
今天有时间,可以完整的听“中国胸部肿瘤大会诊——襄阳站”的MDT直播,第一个病例让
感慨!!!一个非常令人伤感的病例
今天有时间,可以完整的听“中国胸部肿瘤大会诊——襄阳站”的MDT直播,第一个病例让
 希望给没有阅读过的人一些体会(9)
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么样
希望给没有阅读过的人一些体会(9)
本文来自于此书,只是做一些摘抄,分享给深陷迷茫的人。文中观点真实与否,效果怎么样





 显身卡
显身卡





